| ___________________________________________________________ |
|
FEATURED STORIES
CASE 1: Chest pain, High D-Dimer, Barrett's Esophagus
A 68-year-old female from California complained of chest pain that radiated to her back and left arm in April 2015. So she went to the emergency room but an angiogram showed she didn’t have any heart issues. She also complained of bowel issues, gas, chronic acid reflux, shortness of breath and no energy. She was already found to have stomach and heart issues through Fingernail and Tongue Analysis (cracks on the tongue, heartburn, lack of lunulae, etc). Recent blood and imaging tests confirmed it.
In May 2015, a blood test (Table 1) showed she had anemia (low RBC, Hgb), which would partly explain her lack of energy. She also has slight diabetes, indicated by the positive urine glucose. This was confirmed by a subsequent test in June where her fasting glucose was high. Although her CRP level was normal, her homocysteine was already high normal at 7.9, indicating a possible risk for cardiovascular problem. It should ideally be under 7. This is reinforced by her high LDL.
 |
|
In August 2015, another test found that her D-Dimer level was very high at 5250. D-Dimer is typically tested to check for thrombosis or embolism; however, in the absence of a blood clot, as in this case, a high D-Dimer can be used as an indicator of malignancy and increased mortality. In this patient’s case, an endoscopy later found she was showing goblet cell metaplasia consistent with Barrett’s esophagus, a definite risk for esophageal cancer. There was already erosion in her esophagus which is most likely due to her chronic acid reflux and which explains the sharp chest pain she has been experiencing. With her high D-Dimer, elevated homocysteine and the Barrett’s esophagus, she is at an increased risk for cancer. That is why her doctor recommended a CT scan of her abdomen and a test for the cancer markers, CA 19-9 and CEA. In addition to that, she was also diagnosed with mild pulmonary fibrosis, hence her shortness of breath, and calcification of the coronary vessels and splenic artery (possible aneurysm). She is currently taking Digestron, Angiostop and Myomin.
CASE 2: Chronic acid reflux, Barrett's Esophagus
R. S., 73 y/o/m from California, has had a history of digestive issues. In 2007, he had difficulty swallowing and eating. He also lost so much weight. It turned out that he had Barrett’s esophagus, a serious complication of his chronic gastroesophageal reflux disease (GERD). It put him at high risk for esophageal cancer. At that time he took Angiostop, Revivin, Digestron, and Liver Chi. Six months later, he could eat normally and gained his weight back. He continued Digestron and Liver Chi for a year.
 |
|
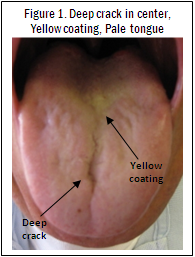
In 2009, he complained of abdominal pain and had difficulty swallowing again. Upon checking, he had a yellow coating and deep crack on his tongue (Figure 1), indicating digestive issues. His tongue was also pale with shiny edges. These two signs are usually associated with ulcers. He did have an ulcer and his digestive problem from 2 years before had recurred, which had him very worried. He has started taking Digestron and Liver Chi again, which helped his condition.
Recently, he said he needed to eat every 3 hours otherwise he gets a feeling of discomfort in his stomach. This is a sign of hypoglycemia and insulin resistance that is why he also experiences an energy crash after every meal. For that, he added Chi Energy, Diabend, OxyPower and Myomin.
CASE 3: Chronic acid reflux, Gastric gland polyp, Intestinal metaplasia
T.C., 58 y/o/m from California, has had acid reflux for more than 10 years despite a very simple and healthy diet. He also walks every day and he always sleeps with his back elevated. But his acid reflux is most likely because, for the last several years, he eats a very late dinner due to his night shift. For the past 10 to 15 years, he has been taking Prilosec and then Nexium, both proton pump inhibitors (PPIs). He was also under the care of a GI specialist at University of California at Irvine. Now he found out that he has a fundic gland polyp, intestinal metaplasia and foveolar hyperplasia. The presence of these conditions already indicates that he is at very high risk for gastrointestinal cancer. The specialist said it was due to the PPIs. Despite his conditions, his doctor cannot do anything clinically yet. If it worsens to cancer, then he can operate and take out his stomach. He is now taking Digestron and Angiostop.
CASE 4: Cracks on the tongue, Family history of stomach cancer
M. S., 62 y/o/f from CA, has cracks on the tongue, teeth marks, and frenula cysts, making her at risk for digestive issues. She relates that her daughter was diagnosed with stomach cancer in May 2015 and died in July. Her mother had pancreatic cancer that metastasized to the stomach.
|
| ___________________________________________________________ |
|
PHYSICAL MARKERS OF DIGESTIVE DISEASE
As with any other diseases, it is important to watch for early signs and symptoms of digestive issues so that prompt action can be taken to prevent the problem from getting worse. Like in Case 1 above, cracks on her tongue already indicated a digestive issue. This was later confirmed by blood and imaging tests. In Case 2 above, he was able to take Angiostop, Digestron, etc. to improve his chronic GERD and Barrett’s esophagus before it can turn cancerous.
Early signs of digestive issues can include:
 |
|
CRACK(S) ON THE TONGUE
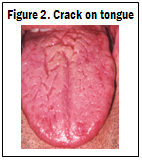
When you check for digestive health, always look for cracking on the tongue, especially on the center (Figures 1 and 2). This usually suggests problems like stomach ulcer. The number of cracks and the depth of the cracks correlate to the number and severity of gastrointestinal (GI) tract or stomach problems, respectively.
YELLOW COATING ON THE TONGUE
A yellow coating on the tongue also signifies digestive problems (Figure 1). When combined with other markers, such as cracks on the tongue, it may signify a more serious digestive issue.
 |
|
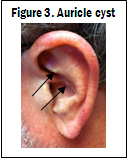
AURICLE CYST
The presence of a cyst (or cysts) in the outer ear is a sign of stomach or esophageal problem. If GERD is also present, the risk for stomach of esophageal cancer is 4 times greater (Figure 3).
BLACK LINES ON FINGERNAILS
Black lines on the fingernails (Figure 4) typically signify bleeding. If there is a crack on the center of the tongue, the bleeding is likely in the stomach. While blood in the stool is an indication of bleeding, minor bleeding may not show up in the stool. About 20% of patients with occult blood have colon cancer; 40% have progressive stomach cancer; and 25% with esophageal cancer.
 |
|
Stomach bleeding associated with stomach ulcers is caused by acid and pepsin secretion. If you have this condition, digestive enzymes will not work. They usually contain Betain HCl, which makes ulcers worse. Betain HCl is only good for the elderly because they lack hydrochloric acid. Some enzymes also have protease, which can aggravate GI mucosa if inflamed. Also, the use of Aspirin, Coumadin or any blood thinners is not recommended for ulcer and gastritis patients as they can increase the risk of bleeding.
The presence of any of these markers are a good indication of a digestive issue especially when they are accompanied by symptoms such as bloating, gas or abdominal pain.
R. Welch, DC from CA, has a male patient in his who had a black line on his fingernail, signifying some kind of bleeding. He did not pay attention to it. Three months later, he told Dr. Welch that he had just gotten out of the hospital. Apparently he was hemorrhaging internally and was vomiting blood due to an ulcer.
|
| ___________________________________________________________ |
GERD/ HEARTBURN/ ACID REFLUX
Gastroesophageal reflux (GERD, also known as heartburn or acid reflux), is a normal physiologic phenomenon experienced intermittently by most people, particularly after a meal, as a result of stomach acid and enzymes refluxing into the esophagus, causing pain and inflammation. Approximately 60% of people will experience some type of acid reflux within a 12 month period.
GERD may be caused when the lower esophageal sphincter fails to function properly. The sphincter normally prevents the stomach acid and enzymes to flow back into the esophagus. It may also be caused by the overgrowth of bacteria, specifically Helicobacter pylori, in the lower esophagus region. To improve GERD and inhibit the H. pylori bacteria, Digestron and GI Chi are recommended.
If left untreated, chronic GERD can lead to problems such as stomach ulcer or Barrett’s esophagus (just as in Cases 1 and 2 above). To improve GERD, Digestron is recommended.
|
|
DIGESTIVE ULCERS
About 95% of ulcers are caused by the H. pylori bacteria. They attack the stomach lining that usually protects you from the acid that digests the food. In the past, stress, spicy foods, smoking and alcohol were thought to cause ulcers. They actually do not; however, they can prevent the ulcer from healing and may worsen it. Ulcers can bleed as they get worse.
For ulcer patients, it is best to eat foods that are easy to digest. Eat foods lower in fat, thereby reducing acid secretion by the stomach. Avoid caffeine, alcohol and pepper, as these will induce acid secretion. Avoid very hot or very cold foods, as they will stimulate parasympathetic nerves and increase acid production. Decrease consumption of sweets and starches and avoid milk as the calcium and protein will increase acid production.
Digestron is recommended for people with ulcer. It has been found to inhibit the H. pylori bacteria as well as repair intestinal mucosa.
|
|
BARRETT'S ESOPHAGUS
When you feel like food is stuck in the throat or it goes down very slowly (especially in chronic GERD patients), and if there’s pain the throat area, a growth or erosion in the esophagus may be the cause. This is typical in Barrett's esophagus, a condition where chronic acid reflux damages the lining of the esophagus. It is a risk factor for esophageal cancer.
Besides symptoms, a dark brown or yellow tongue coating, teeth marks on the tongue as well as a cyst in the auricle may indicate esophageal cancer risk.
Additionally, if you have GERD and an ulcer and suddenly experience sharp abdominal pain, this may indicate cancer.
For Barrett’s esophagus, take Digestron with Angiostop. Digestron will help repair damage to the esophageal lining and neutralize GERD. Angiostop will keep abnormal cells from becoming malignant (like in Case 2 above).
J. Florendo, DC from NV, has a male patient in his 40s with Barrett’s esophagus. From March to May, 2007, 2 continuous endoscopies found a tumor in his throat. He then started taking Angiostop. After 6 months, his physician said he has no tumor anymore.
A. Sayler, CN in FL, has a 49 y/o/m patient, David, who had stage 4 esophageal cancer for 3 ½ years. At the time of diagnosis, he underwent chemo and radiation and was told that he had 1 year to live. Then he took Angiostop, Revivin, and Reishi Spore. It has been 5 ½ years now and he is cancer-free. His number is (813) 334-3737.
|
| ___________________________________________________________ |
|
DIGESTRON for GERD, STOMACH ULCER, GASTRITIS, BARRETT'S ESOPHAGUS
Digestron is not an enzyme product. It is an herbal supplement that has multiple functions for the digestive system:
- It increases secretion of digestive enzymes and reduces bloating and gas.
- It also adjusts stomach and intestinal involuntary muscle contractions for better digestion.
- It inhibits the
H. pylori bacteria for ulcers and GERD
- It also strengthens and repairs stomach and intestinal membranes that might have been damaged through GERD and other digestive disorders.
People who are skinny or have diarrhea often can take digestive enzymes. However, if no improvement is seen after one month, they should stop taking the enzymes and switch to Digestron instead. Nowadays, taking digestive enzymes is the first recourse when people feel bloated. This is not always a smart thing to do, especially if it becomes habitual. It is important to know the underlying cause first because long-term use of digestive enzymes can make the pancreas lazy and stop producing its own enzymes (a process called feedback inhibition). Besides, the pancreas can eventually become insensitive, creating a high risk for developing insulin resistance and diabetes. People with digestive problems should avoid grease, cold drinks, and sweets. These foods, especially the sweets, curb enzyme production in the stomach and pancreas.
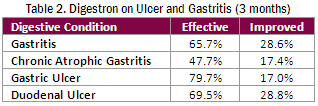
Scientific studies show that Digestron is effective for such conditions as gastritis and ulcers. In 952 cases of these conditions, Digestron was overall effective in 59% of the cases within 3 months of use while improvement was seen in 29% of the cases (Table 2).
 |
|
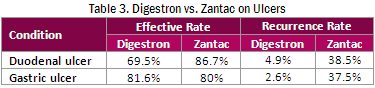
In another study, Digestron was compared to Ranitidine (generic for Zantac), a histamine H2- receptor antagonist used to treat ulcers in the stomach and intestines by reducing the acid production by the stomach. Results of the study indicate that Digestron’s effectiveness for duodenal and gastric ulcers is comparable to that of Zantac; however, Digestron is much better at reducing recurrence (Table 3).
 |
|
CASE REPORTS:
L. K., a 45 year-old-female from NY reported that she had severe digestion problems for more than 10 years. She took digestive enzymes for many years but still had diarrhea. She was underweight and had no energy. Dr. Chi suggested that she stop taking digestive enzymes and start taking Digestron instead. After 3 days she no longer had diarrhea, her energy increased, she started to gain weight and her face color went back to normal. Four months later she decided to try digestive enzymes again. On the first day she took digestive enzymes, she started to have diarrhea. She always had diarrhea every time she took digestive enzymes. So now she knows to take only Digestron. This case illustrates that digestive enzymes may not work even for people who are underweight and have diarrhea.
A.T., 52 y/o/f from CA, has had GERD for about 5 years and abdominal bloating for 2 years. She used Digestron, Debile, Asparagus Extract, and Vein Lite. After only 3 days, the bloating is completely gone while her GERD has noticeably subsided.
A. Sayler, CN from FL, reports on S.A., a 42 y/o/f who has been suffering from GERD for 20 years. She has used all kinds of drugs. It was only after she started taking Digestron that she felt much improvement. After 3 months on Digestron, her reflux has improved significantly. She already has erosion in the throat. Now it is much better.
|
| ___________________________________________________________ |
|
SUMMARY
If you already have GERD or acid reflux, take Digestron right away to help protect your esophagus, intestinal and stomach linings. This will also help avoid damage to your espohagus that can lead to Barrett's esophagus. If you have a history of GERD and feel that there is something blocking your esophagus and you have trouble swallowing, take Angiostop. Most likely you already have Barrett's esophagus and need to make sure that it doesn't develop into cancer.
If you do not have the typical symptoms of digestive issues like bloating, gas or abdominal pain, look for cracks on the tongue, cyst in the auricle or black lines on the fingernails. These are early markers of digestive problems. Check for bleeding especially when you have black lines on the fingernails. Often blood may be seen in the stool or the stool itself is dark colored.
In our next issue, we will continue our digestive series with discussion on colon conditions, leaky gut syndrome and Celiac disease.
|
| ___________________________________________________________ |
TRY THIS TODAY
DIGESTRON
OR CALL TOLL-FREE TO ORDER
(800) 457-5708
|
|
|
UPCOMING EVENTS
|
Please visit our booth at these conventions.
AARM CONFERENCE
October 2-4
Semiahmoo Resort
Blain, WA
Booth #208
NEW LIFE EXPO
October 16-18
Hotel Pennsylvania
Penn Plaza Pavilion
New York, NY
Booth 115
Attend Dr. Chi's FREE lecture on Saturday, October 17 at 3:00 pm
PACIFIC SYMPOSIUM
Oct 30 - Nov 1
Catamaran Resort Hotel
San Diego, CA
Booth #67
For more information, please call
(714) 777-1542 |
|
PATIENT SCREENINGS IN YOUR AREA
|
|
Interested in a Fingernail and Tongue Analysis screening by Dr. Chi? He may be in your area! Check out the schedule below.
BROOKLYN, NY
October 19
Dr. Yury Dikansky
(718) 236-4057
October 20
Dr. Jeffrey Weber
(718) 376-2300
October 21
Dr. Irina Lelchuk
(718) 648-4545
Please call the above sponsors for details and scheduling.
PRIVATE CONSULTATIONS
BLAINE, WA
October 1-3
LAS VEGAS, NV
December 10-12
Call (714) 777-1542 to make an appointment for these private consultations.
|
|
CONTACT US
|
Chi's Enterprise, Inc.
1435 N. Brasher Street
Anaheim, CA 92807
(714) 777-1542
(800) 457-5708
postmaster@chi-health.com
www.chi-health.com
OFFICE HOURS
Monday to Friday
8:00 am - 5:00 pm |
|
FOLLOW US
|


|
|
